
Catherine Kaufman is a staff writer for Brief Policy Perspectives and a second-year MPA student.
Conversion therapy, or practices claiming to “change a person’s sexual orientation, change their gender identity or expression, or lessen their same-sex sexual attraction,” has long been discredited and considered dangerous for those who are subjected to it. These practices have been largely proven ineffective at actually changing a child’s future sexual orientation or gender identity—qualities that are now not even classified as a disease or mental disorder that needs to be “fixed.” And those who have experienced conversion therapy have been shown to have an increased risk of suicide, depression, drug use, and STIs, among other serious harm. The United Nations has even called for a global end to conversion therapy for minors, stating that it “may amount to torture.”
Even still, the practice to “cure” LGTBQ+ individuals, particularly minors, is more prevalent today than many realize. The UCLA Williams Institute estimates that, as of 2019, about seven percent of LGBTQ+ adults have been subjected to conversion therapy, and around 16,000 more youth in states where the practice is legal will experience it before they become adults. And though acceptance of homosexuality and other identities is rising in the United States, the Republican Party platform (holding from 2016) continues its veiled endorsement of conversion therapy through its support of “the rights of parents to determine the proper medical treatment and therapy for their minor children,” among other anti-LGBTQ+ language.
Recognizing the harm being done, twenty-one states, the District of Columbia, and Puerto Rico have some type of ban on conversion therapy for minors from licensed professionals (the North Carolina ban applies only to the use of state funds). These bans are quite popular among US citizens across age, region, and rural/urban classifications, with a majority (56%) believing that conversion therapy on youth by mental health practitioners should be illegal, holding steady across age, region, and rural/urban classifications. Though the majority of these states were controlled by Democratic legislatures at the time of passage, there are three notable exceptions besides Puerto Rico, with two taken through executive action (see Table 1 below).
But do these bans, as written, actually work to prevent harmful conversion efforts from taking place? To answer that question, we first need to look at the text of the bans themselves.
Text of Conversion Therapy Bans
State lawmakers often do not have the time or staff to draft each bill that they propose. Instead, they often use model text or sample legislation to increase productivity and lower legislative costs, typically drawing either from other states or from interest groups. A key sample legislation used in conversion therapy bans was put out in 2015 by the Human Rights Campaign (HRC) and the National Center for Lesbian Rights (NCLR), which combines and builds on best practices from already-introduced legislation and provides a model for future legislation.
Most states have stuck quite closely to this text, whether by relying on the sample legislation itself or looking at bans already enacted by other states. All of the twenty-one states plus DC and Puerto Rico, for example (with the exception of North Carolina), use licensing to restrict the practice of conversion therapy, stating that any licensed professional (or licensing agency, in the case of Executive Orders) will be subject to disciplinary action if they administer conversion therapies to minors while acting in their licensed capacity. Definitions of conversion therapy and licensed professional differ slightly, though they refer to essentially the same practice.
There are some key differences between the states, however, that could impact the functionality of the bans. The model text recommends three optional sections that can extend the way these bans are enacted or enforced in addition to the licensing requirements: protect vulnerable adults as well as minors from conversion therapy, outlaw consumer fraud related to conversion therapy (i.e., making it illegal to claim that the service will change a person’s sexual orientation or gender identity because it has been proven not to change anything), or prohibit the use of state funds for conversion therapy. Table 1 indicates which states, if any, have exacted these provisions into their respective bans:
Table 1: Conversion Therapy Bans by U.S. State/Territory
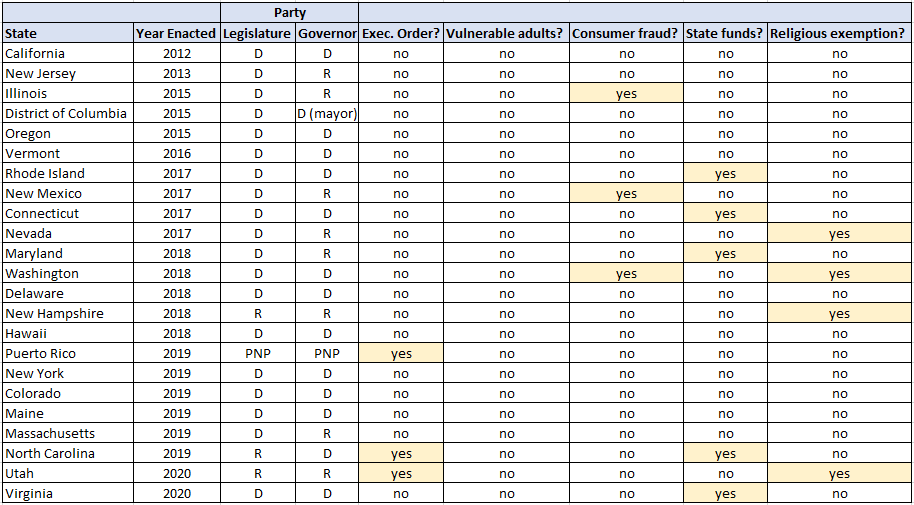
Another provision that multiple states have begun adding since 2017 that is not included within the model text is to specifically exclude those acting in a religious or familial capacity from those who cannot perform conversion therapy. Notably, these exemptions are already built into every state’s ban if they are not acting in a licensed capacity. These explicit exclusions, three of the four of which exist in states with a Republican-controlled branch, were thus likely added to preempt any criticism or claims of religious discrimination from their constituents.
Are the Bans Effective?
The inherent problem with these bans, and even the model legislation, is that they only preclude conversion therapy that takes place in a licensed, “professional” environment. Most people who have been subjected to conversion therapy have not received it from a licensed professional. According to a study conducted by the UCLA Williams Institute, 81% of those who experienced conversion therapy as minors received it from a religious leader and only 31% from a health care provider. While most states require pastoral counselors to become licensed professionals (commonly as a marriage and family therapist or a clinical professional counselor), many religious leaders are not officially licensed, thus exempting them from any states’ ban on conversion therapy, likely doing little to prevent 81% of the study’s cases.
However, states have limited options to outlaw conversion therapy besides revoking licenses, and they must be specifically aimed as not to overstep on freedoms of religious belief and speech—recently, for instance, a federal court struck down a southern Florida conversion therapy ban by stating that it was too broad and violated First Amendment rights (a ruling the American Psychological Association stated was “wrong-headed and may well result to harm to patients, especically minors who are often subjected to this type of therapy against their will”). Conversion therapy is also difficult to pin down, with rebranding around personal freedom and different language, so legal bans may be unable to achieve the level of specificity needed to end the practice.
The optional sections recommended by the model text, then, become perhaps the most effective tools to combat the practice. The consumer fraud and state funds sections move enforcement away from licensing and toward financial implications, limiting the profitability of conversion therapy for anyone, licensed or not, who practices it. If a ban on conversion therapy at a national level, for example, focuses on consumer fraud, it may be far more effective than one that focuses on the more state-level issue of licensing practitioners.
Ultimately, these bans have likely helped and will continue to help save LGBTQ+ youth from some methods of conversion therapy while sending a message to practitioners and to parents and guardians that the practice is ineffective and can cause long-term damage. As LGBTQ+ rights are more widely recognized and protected in other parts of society, and LGBTQ+ youth feel safe and accepted when coming out, hopefully demand for the service will drop along with instances of conversion therapy.
